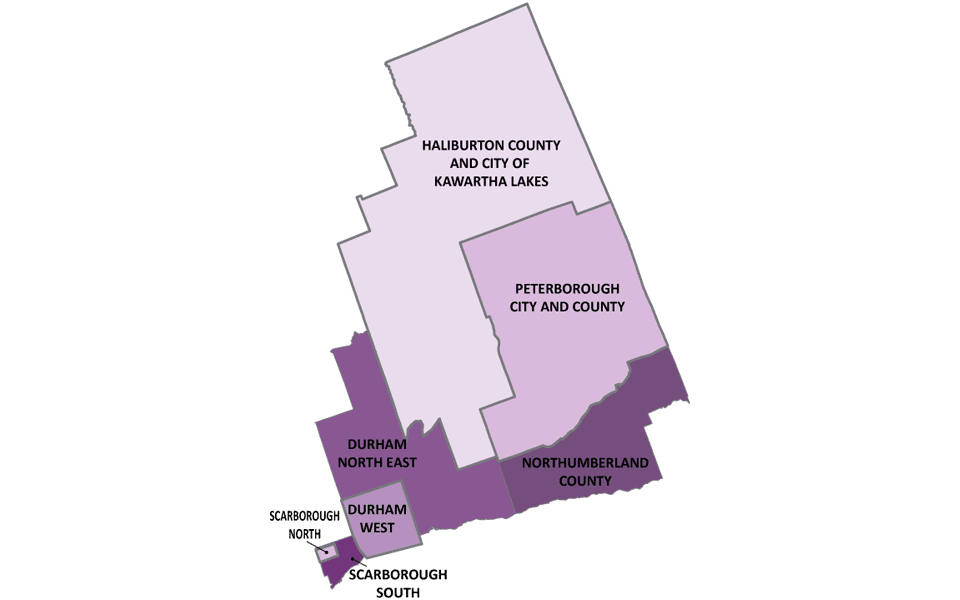
Région de Centre-Est
Nous sommes Santé à domicile Ontario(S’ouvre dans un nouvel onglet) , un seul organisme qui coordonne la prestation des services de soins à domicile et en milieu communautaire, de placement en foyer de soins de longue durée et de renvoi vers les services communautaires.
Renseignements concernant les patients et renvois
310-2222
Sans frais au Canada:1 800 263-3877
Fax:1 855 352-2555
TTY:711
Visitez le site Web lignesanté du Cente-Est
Emplacements des bureaux du Centre-Est
-
Whitby
920 Cour Champlain
Whitby, ON, L1N 6K9
-
Scarborough
100 Place Consilium
Bureau 801
Scarborough, ON, M1H 3E3
-
Port Hope
151A, chemin Rose Glen
Port Hope, ON, L1A 3V6
-
Lindsay
370, rue Kent Ouest
Lindsay, ON, K9V 6G8
-
Campbellford
119, rue Isabelle
Unité 7
Campbellford, ON, K0L 1L0
-
Peterborough
700, avenue Clonsilla
Bureau 202
Peterborough , ON, K9J 5Y3
-
Haliburton
73, rue Victoria
Boîte postale 793
Haliburton, ON, K0M 1S0
Compliments et Inquiétudes
Veuillez transmettre vos commentaires à votre coordonnateur de soins. Vous pouvez aussi communiquer vos compliments ou préoccupations d’une des manières suivantes :
Par courriel : CE.patientrelations@ontariohealthathome.ca
Téléphone : 1-800-263-3877 poste 2273
Par la poste : Santé à domicile Ontario
Compliments et inquiétudes
Bureau de Whitby
920 Cour Champlain
Whitby, ON L1N 6K9
Documents d’accessibilité
- Accessibility Policy
- Annual Accessibility Status Report 2025
- Multi-Year Accessibility Plan – 2025
- AODA 2025 Compliance Report Submission
Avis de non‑responsabilité : Les catalogues sont disponibles en anglais seulement.
Publications
- Fiche d’information sur les Cliniques de soins infirmiers communautaires
- Guide de bienvenue
- Guide des placements dans les foyers de soins de longue durée
- Infirmières et infirmiers en santé mentale et en toxicomanie dans les écoles
- Infirmières et infirmiers en santé mentale et en toxicomanie | Affiche
- Votre lien aux soins
Forms
Nous éprouvons actuellement des problèmes d’accès à la liste de résultats de recherche de la Bibliothèque de documents. Entre-temps, nous vous demandons d’utiliser la version anglaise de la Bibliothèque (opens in a new tab) de documents pour accéder aux documents. Nous regrettons tout inconvénient que cela peut vous causer et nous vous remercions de votre patience.
| Title | Summary | Tags | Categories | Last modified date | Link | hf:doc_tags | hf:doc_categories |
|---|---|---|---|---|---|---|---|
| Demande d’évaluation | Tél. : 800-263-3877 | Central East | Formulaire | September 11, 2025 | central-east-fr | formulaire | |
| Évaluation de l’état de santé – Santé à domicile Ontario | Ce formulaire doit être utilisé pour effectuer l’évaluation de l’état de santé exigée en vertu de la Loi de 2021 sur le redressement des soins de longue durée lorsqu’une personne présente une demande de détermination de l’admissibilité à l’admission à un foyer de soins de longue durée. L’évaluation exigée porte sur la santé physique et mentale du demandeur ainsi que sur ses besoins en matière de traitements médicaux et de soins de santé. Cette évaluation doit être faite par un médecin ou un infirmier autorisé. | Central, Central East, Central West, Centre-Toronto, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North Simcoe Muskoka, South East, South West, Toronto Central, Waterloo Wellington | Formulaire | September 11, 2025 | central-fr central-east-fr central-west-fr centre-toronto champlain-fr erie-st-clair-fr global-fr hamilton-niagara-haldimand-brant-fr mississauga-halton-fr north-simcoe-muskoka-fr south-east-fr south-west-fr toronto-central-fr waterloo-wellington-fr | formulaire | |
| Formulaire de demande d’une trousse de gestion des symptômes pour les soins en fin de vie | Veuillez prêter une attention particulière aux choix du moment et de l’endroit où la trousse de gestion des symptômes sera mise en service (par exemple, si le pronostic de survie est de moins de six mois ou que l’on envisage une détérioration rapide de la santé du ou de la patient.e). | Central East, Champlain, Sud-Est | Formulaire | July 28, 2025 | central-east-fr champlain-fr sud-est | formulaire |