Région de Centre
Nous sommes Santé à domicile Ontario(S’ouvre dans un nouvel onglet) , un seul organisme qui coordonne la prestation des services de soins à domicile et en milieu communautaire, de placement en foyer de soins de longue durée et de renvoi vers les services communautaires.
Renseignements concernant les patients et renvois
1 833 515-1234
Sans frais au Canada :1 888 470-2222
Télécopieur :416 222-6517 or 905 952-2404
TTY :711
Visitez le site Web lignesanté Centre

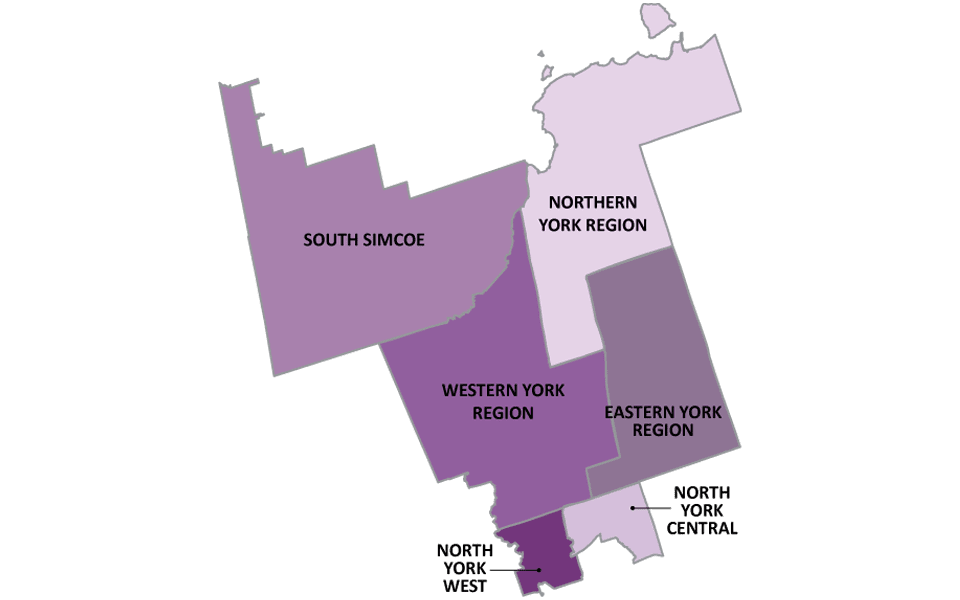
Emplacements des bureaux du Centre
-
Markham(Corporate Office)
11, Allstate Parkway, bureau 500
Markham, ON, L3R 9T8
-
Newmarket
1100, rue Gorham, unité 1
Newmarket, ON, L3Y 8Y8
-
North York
45, avenue Sheppard Est, bureau 600
North York, ON, M2N 5W9
Compliments et Inquiétudes
Veuillez transmettre vos commentaires à votre coordonnateur de soins. Vous pouvez aussi communiquer vos compliments ou préoccupations d’une des manières suivantes :
Par courriel : central.patientexperience@ontariohealthathome.ca
Téléphone : 905 948-1872 poste 7230
Par la poste : Santé à domicile Ontario
Gestionnaire, Expérience du patient
11, promenade Allstate, bureau 500
Markham, ON L3R 9T8
Documents d’accessibilité
Publications
- Accès Soins Renseignements pour les patients et les familles
- Cliniques de soins infirmiers communautaires
- Foyers de soins de longue durée – lignesantecentre.ca
- Guide de bienvenue
- Guide des placements dans les foyers des soins de longue durée
- Liste des foyers de soins de longue durée
- Votre lien aux soins
Formulaires
La plupart des formulaires sont disponibles en anglais seulement. Veuillez utiliser le répertoire centralisé des formulaires(S’ouvre dans un nouvel onglet) et les filtres par secteur pour trouver l’information. De l’aide ou des formats accessibles sont offerts sur demande.
| Title | Summary | Tags | Categories | Link | hf:doc_tags | hf:doc_categories |
|---|---|---|---|---|---|---|
| Formulaire de renvoi vers les services auxiliaires de santé dans les écoles | Les conseils scolaires qui font appel aux services de conseillers en ergothérapie, physiothérapie et orthophonie sont tenus de fournir un rapport et la signature de chaque conseiller. *Les formulaires de renvoi qui manquent de renseignements ne seront PAS traités. | Centre | Formulaire | centre | formulaire | |
| Évaluation de l’état de santé – Santé à domicile Ontario | Ce formulaire doit être utilisé pour effectuer l’évaluation de l’état de santé exigée en vertu de la Loi de 2021 sur le redressement des soins de longue durée lorsqu’une personne présente une demande de détermination de l’admissibilité à l’admission à un foyer de soins de longue durée. L’évaluation exigée porte sur la santé physique et mentale du demandeur ainsi que sur ses besoins en matière de traitements médicaux et de soins de santé. Cette évaluation doit être faite par un médecin ou un infirmier autorisé. | Centre, Centre-Est, Centre-Ouest, Centre-Toronto, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, Nord-Est, Nord-Ouest, Simcoe Nord Muskoka, Sud-Est, Waterloo Wellington | Formulaire | centre centre-est centre-ouest centre-toronto champlain-fr erie-st-clair-fr global-fr hamilton-niagara-haldimand-brant-fr mississauga-halton-fr nord-est nord-ouest simcoe-nord-muskoka sud-est waterloo-wellington-fr | formulaire |